Pediatric Cardiac Examination
The paediatric cardiac exam in the ED aims to rapidly identify children with congenital heart disease, heart failure, shock, arrhythmia or carditis. It combines focused history, vital signs, assessment of perfusion, and careful auscultation.
Focused Cardiac History
Useful ED screening questions include:
- Family history of congenital heart disease, sudden cardiac death, cardiomyopathy, arrhythmias.
- Pregnancy/perinatal history: maternal diabetes, infections, medications, prematurity, NICU stay.
- Feeding history in infants: poor feeding, sweating when feeding, prolonged feeds, failure to thrive.
- Breathlessness: tachypnoea, recurrent chest infections, difficulty keeping up with peers.
- Cyanosis: central (tongue, lips) vs peripheral; episodes during crying/feeding.
- Syncope or presyncope, especially exertional or associated with palpitations/chest pain.
- Exercise tolerance in older children: inability to run/play normally, early fatigue.
- Past history of rheumatic fever, Kawasaki disease, known heart disease, or cardiac surgery.
- Medications (including stimulants, antiepileptics, chemotherapy).
Vital Signs & Perfusion
Record and interpret age-appropriate vitals (see your paeds vitals page):
- Heart rate (tachycardia / bradycardia, rhythm regular vs irregular).
- Respiratory rate and work of breathing (heart failure often presents with tachypnoea).
- Blood pressure – ideally four-limb BP in suspected coarctation.
- Oxygen saturation – pre- and post-ductal (right hand vs foot) if cyanotic heart disease suspected.
- Temperature (fever raises suspicion for myocarditis, pericarditis, rheumatic carditis, sepsis).
Assess perfusion:
- Capillary refill time (central and peripheral).
- Skin colour and temperature: mottling, cool peripheries, central cyanosis.
- Hepatomegaly – an important sign of paediatric heart failure.
- Urine output (if known) and level of consciousness.
General Inspection
- Growth: underweight, small for age, or faltering growth can reflect chronic cardiac disease.
- Cyanosis: lips/tongue (central) vs hands/feet (peripheral); clubbing in chronic conditions.
- Respiratory distress: nasal flaring, retractions, grunting.
- Chest wall: visible precordial activity, deformity (pectus excavatum), surgical scars.
- Dysmorphic features associated with syndromes (e.g. Down syndrome with AVSD).
- Peripheral oedema (rare in small children, more common in adolescents).
Pulses, JVP & Precordium
Pulses & Blood Pressure
- Palpate brachial and femoral pulses in infants; look for delay or absence (coarctation).
- In older children, check radial and femoral pulses simultaneously for radio-femoral delay.
- Assess pulse volume and character (bounding, thready, collapsing).
- Measure arm and leg BP if coarctation is suspected (leg BP lower than arm is abnormal).
JVP / Neck Veins
- JVP assessment is harder in small children but gross distension suggests right heart failure or tamponade.
Precordial Palpation
- Locate the apex beat/PMI (usually 4th–5th ICS mid-clavicular in children) – is it displaced?
- Feel for heaves (ventricular hypertrophy) with the heel of your hand at left sternal edge.
- Feel for thrills (palpable murmurs) at the valve areas and along left sternal border.
- Note any tenderness or chest wall abnormalities (consider trauma, costochondritis).
Auscultation of the Heart
Use both the diaphragm (high-pitched sounds) and bell (low-pitched sounds). Listen in a quiet environment with the child as calm as possible.
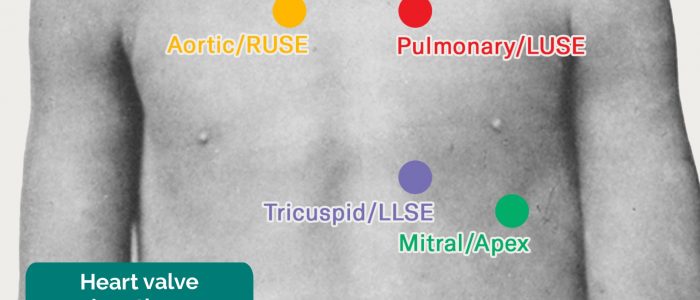
- Aortic area – right 2nd ICS parasternal.
- Pulmonic area – left 2nd ICS parasternal.
- Tricuspid area – left lower sternal border.
- Mitral area – apex (5th ICS mid-clavicular, more lateral in older children).
- Back and axilla – to follow radiation of murmurs (e.g. PDA to back, MR to axilla).
Heart Sounds
- S1: closure of mitral/tricuspid; best at apex. Usually single and normal.
- S2: closure of aortic/pulmonic; normally splits with inspiration in older children.
- Wide, fixed split S2: classic for atrial septal defect (ASD).
- S3: may be normal in children/young adults; with symptoms it can indicate heart failure.
- S4: usually pathologic; suggests stiff ventricle, hypertrophy or reduced compliance.
Murmurs – Innocent vs Pathological
Key features of a likely innocent/physiological murmur:
- Soft (grade 1–2/6), systolic only, short, musical or vibratory.
- Best heard at left sternal border, no radiation.
- Normal S2, no clicks, no added sounds.
- No symptoms (normal growth, exercise tolerance, no cyanosis).
Features suggesting a pathological murmur:
- Harsh, loud (> 3/6), pansystolic, diastolic or continuous murmur.
- Abnormal S2 (single, widely split, loud P2).
- Radiation to back, neck or axilla.
- Associated symptoms: cyanosis, failure to thrive, syncope, chest pain, heart failure signs.
Common Pediatric Cardiac Abnormalities – Exam Clues
| Condition | Key Clinical Findings |
|---|---|
| Ventricular Septal Defect (VSD) |
|
| Atrial Septal Defect (ASD) |
|
| Patent Ductus Arteriosus (PDA) |
|
| Tetralogy of Fallot (TOF) |
|
| Coarctation of the Aorta |
|
Key ED Investigations
- Pulse oximetry: pre- and post-ductal saturations in suspected congenital heart disease.
- ECG: rhythm, rate, axis deviation, chamber hypertrophy, conduction abnormalities, QT interval.
- Chest X-ray: heart size, pulmonary vascularity, lung pathology, characteristic silhouettes (boot-shaped heart, egg-on-a-string, etc.).
- Blood tests: FBC, CRP, troponin, BNP/NT-proBNP, electrolytes if myocarditis/heart failure suspected.
- Echocardiography: usually done by paediatric cardiology/echo service; arrange urgently if unstable.
Valve & Auscultation Areas
Summary
The paediatric cardiac exam in the ED focuses on recognising children who are unstable or have significant structural or functional heart disease. A structured approach – history, vitals, perfusion assessment, precordial exam and auscultation – plus judicious use of ECG, CXR and echocardiography, allows timely diagnosis and referral. When in doubt, observe, repeat the exam, and escalate early.